Published in Criminal Law by Chris Eskew on April 29, 2016.

It’s no secret that the use of heroin in the U.S. has been increasing at an alarming rate. Many, including the CDC, are calling it an epidemic. As the number of heroin users has escalated, so too have heroin-related overdose deaths. Between 2002 and 2013, the rate of heroin-related overdose deaths has increased by more than 4X. In 2014, more than 10,500 people died as the result of heroin overdoses.
What is causing the heroin epidemic?
Heroin use – and overdose deaths and hospitalizations – are on the rise for two major reasons. Prescription opioid abuse (mostly due to widespread over prescribing) and the low cost, wide availability of heroin.
Overprescribing created the public impression that prescription opioids do not carry a high risk of addiction and are not dangerous drugs. This is absolutely not the case. Since 1999, prescription opioids sales in the U.S. have nearly quadrupled and so too have opioid overdose deaths.
But prescription drug addiction is expensive and access to drugs can be difficult to come by. Heroin, on the other hand, is cheaper then it’s ever been before and relatively easy to find. So prescription opioid users have been switching to heroin in droves.
Over 50% of recent heroin addicts report that they began their opioid use through the abuse of prescription opioid medications.
The result? Overdose deaths from heroin and prescription opioids have more than quadrupled since 1999. Nearly 78 people die from overdoses of every day.
What’s more, heroin’s body count could be significantly higher as heroin related deaths are very often undercounted. This happens for two key reasons. One, reporting procedures vary greatly from state to state.
Two, and perhaps more often overlooked, heroin metabolizes into morphine very quickly in the body, thus making it difficult to correctly determine the presence of heroin.
Medical examiners are typically reluctant to rule a death as heroinrelated without the presence of 6-monoacetylmorphine (known as 6MAM) – the unique heroin metabolite that quickly metabolizes to morphine. Heroin (diacetlymorphine) is broken down into 6MAM in as little as 44 minutes. 6MAM is thought to be detectable for no more than 6 hours after taking heroin, and is often metabolized in 24 hours.
Therefore, many heroin related deaths are attributed to other opioids.
Stronger, Cheaper, More Deadly
The second part of the heroin epidemic equation is the price, purity and availability of heroin. The heroin of today is drastically different from the heroin of the 1980’s. What is on the street is significantly higher in purity and sold at a much, much lower price.
For example, in 1981, one gram of pure heroin sold for nearly $6,000 and the expected purity at the street level was less than 11%. In 2013, that same gram of pure heroin sold for $552 and users could expect a purity of nearly 40%.

Why does this price and purity change matter? For one, it creates easier and cheaper access to a much more potent drug. Two, studies have shown that this decrease in price directly affects heroin overdoses. Recent analysis of the United States has shown that for every $100 decrease in the price of heroin there is a 2.9% increase in heroin overdose hospitalizations.
Who Is Using Heroin?
The heroin epidemic – and the panic surrounding it – is real. But heroin isn’t a new drug, it’s been around for a long time. In fact, in the 1890’s Bayer marketed heroin as a cough medicine for children! After other proclaimed epidemics in inner-city neighborhoods during the 1960’s, 70’s and 80’s, heroin seemed to slip from the nation’s collective consciousness.
So what changed? The users.
In decades past, heroin use was associated with poor, economically struggling minorities and overdoses always seemed to happen . Todays epidemic sees more and more younger, affluent, white users in suburban and rural areas – and overdose events are happening in public places like restaurants, libraries, buses and at work.
Emergency Department Visits by Age Group
Emergency Department Visits by Race
Click the “start graph” link below, then either scroll through the animation or click the navigation dots on the right to see the race data.
What Exactly Is Heroin? How is it Made, How is Sold and How Is It Used?
Heroin is a highly addictive, illegal opioid drug derived from the Poppy plant. At the street level it is sold in “stamp bags”, typcially in increments of 100 mg. Heroin can be injected, insufflated (snorted), or smoked. According to the SAMHSA, 70% of primary heroin admissions to drug treatment centers reported injection as the route of administration, and 25% reported inhalation.
How Does Heroin Affect the Body?
After an intravenous injection of heroin, users report feeling a surge of euphoria (“rush”) accompanied by dry mouth, a warm flushing of the skin, heaviness of the extremities, and clouded mental functioning. Following this initial euphoria, the user goes “on the nod,” an alternately wakeful and drowsy state. Users who do not inject the drug may not experience the initial rush, but other effects are the same.
What Happens when someone overdoses on Heroin?

When a user overdoses on heroin (or another opioid drug), the brain signals that tell them to breath slow way down and the brainstem’s ability to automate the breathing process is blocked. This is known as respiratory depression. Then, when they fall asleep, they simply stop breathing.
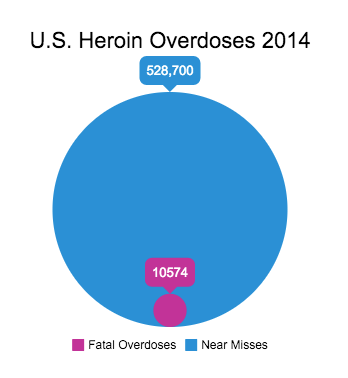
This event is not always fatal, almost 22 percent of heroin users will suffer a near miss – an overdose event where you fall asleep and almost don’t wake up. In fact, it’s so common that some experts estimate that for every fatal heroin overdose, there are as many as 50 near misses. That would mean that in 2014, there were 528,700 non fatal heroin overdose events in the U.S.!
Researchers are finding too, that many heroin deaths are aren’t simple overdoses – but the result of the interactions of the drugs used as adulterants. Dealers have always cut pure heroin with both adulterants and inert substances to augment the effects of the drug as well as dilute the purity and increase profits. The result is often an extremely deadly cocktail of stimulants, depressants and various other drugs and substances.
Common Adulterants found in heroin:
- Quinine (an antimalarial drug used for rush effect)
- Acetaminophen (can be used to disguise poor quality heroin)
- Cocaine (the affectionately known ‘speedball’)
- Caffeine (causes heroin to vaporize a lower temperature)
- Strychnine (for effect on the rush)
- Fentanyl (extremely potent opioid – because apparently regular heroin isn’t strong enough for some people)
- Procaine or Lidocaine (for effect on the rush)
- Benzodiazepines (tranquilizers commonly referred to as “Benzos” – Xanax and Valium been notable examples)
- Dextromethorphan (cough syrup compound)
- Dormice (sleep aid)
Common Diluents (Inert Substances) used to cut heroin:
- Mannitol (baby laxative)
- Flour
- Talcum Powder
- Starch
- Powdered Milk
- Sugar
- Chalk
- Vitamin b12
Where does Heroin in the U.S. come from?
The overwhelming majority of heroin sold in the United States today comes from Mexico and South America.
The table below shows the percentage of where heroin seized by the DEA from 1977 to 2011 originates.
How Does Heroin Puts Users at Risk of HIV Infection?
Because most heroin users administer the drug intravenously (around 75% of users), it’s use puts them at an especially high risk of contracting HIV or Hepatitis B & C. Consider this:
- Over HALF of heroin users who test positive for HIV are unaware of their status.
- Over Half of all heroin addicts have admitted to sharing needles at some point.
- Almost 10% of new HIV infections are from needle-sharing heroin users.
- In 2010, intravenous drug users (IDU) accounted for 53% of new Hepatitis C infections in the U.S.
- Each IDU infected with hepatitis C is likely to infect 20 other people.
What Is Being Done To Fight The Heroin Epidemic?
Recently, President Obama unveiled a two-pronged plan to combat the heroin and opioid abuse epidemic. The plan earmarks more than $1 billion in funding for education, treatment, harm reduction programs across the nation. The plan will also double the amount of doctors prescribing buprenorphine -used to treat opioid addiction – and increase access to Naloxone – a life saving drug in the event of an overdose.
Perhaps most notably, it will focus on improving training for doctors prescribing opioid medication.
But more needs to be done. Currently health care providers receive very limited education about how to appropriately prescribe opioid medication and fewer than 10% of medical schools offer any sort of instruction on addiction treatment. According to the National Heroin Task Force report , as many as 80% of attending doctors rate their med school education on chronic pain as inadequate. Currently, only ten states (Connecticut, Delaware, Iowa, Kentucky, Massachusetts, New Mexico, Tennessee, Utah, West Virginia, and Maryland) have legislation requiring prescriber training in pain management and addiction as well as clinical guidelines to reduce abuse.
